

Featured Resources
-
STORM Therapeutics: From Lead to Pre-Candidate Nomination in 18 Months

STORM Therapeutics: From Lead to Pre-Candidate Nomination in 18 Months
Case study
📣From lead to pre-candidate nomination in 18 months. Explore the STORM Therapeutics case study






Discover precise insights into brain neurochemistry with Sygnature Discovery's in vivo microdialysis and cOFM services. With over 20 years of expertise, we design bespoke studies that reveal how compounds modulate neurotransmitter systems in health and disease. Using UHPLC/HPLC with electrochemical detection or mass spectrometry, we deliver robust PK/PD data to support confident CNS decision making.




July 30, 2015

Inobrodib, an exciting, first-in-class oral anti-cancer drug in clinical development by CellCentric, was collaboratively designed, synthesised and supported on its pre-clinical journey by an integrated project team at Sygnature Discovery. Inobrodib is now showing promising results in Phase I and II trials for multiple myeloma and other cancer types.

In drug discovery, generating targets is no longer the challenge. The real question is how to identify the few worth investing months of research and significant resources to pursue. Hear expert perspectives on how AI, pathway analysis and scientific expertise are shaping modern target identification.
July 7, 2026

Stay up to date with the latest company updates, milestones, and announcements.

Explore upcoming conferences and scientific meetings where you can connect with our team.

At Sygnature Discovery, we deliver world-leading drug discovery solutions to accelerate your compound from idea to clinic.

Our leadership team brings diverse experience and insight, driving collaboration and innovation across drug discovery.

Explore careers at Sygnature Discovery and join a global team committed to science, collaboration, and integrity.
Inobrodib, an exciting, first-in-class oral anti-cancer drug in clinical development by CellCentric, was collaboratively designed, synthesised and supported on its pre-clinical journey by an integrated project team at Sygnature Discovery. Inobrodib is now showing promising results in Phase I and II trials for multiple myeloma and other cancer types.
At Sygnature Discovery, we deliver world-leading drug discovery solutions to accelerate your compound from idea to clinic.
Our leadership team brings diverse experience and insight, driving collaboration and innovation across drug discovery.
Explore careers at Sygnature Discovery and join a global team committed to science, collaboration, and integrity.
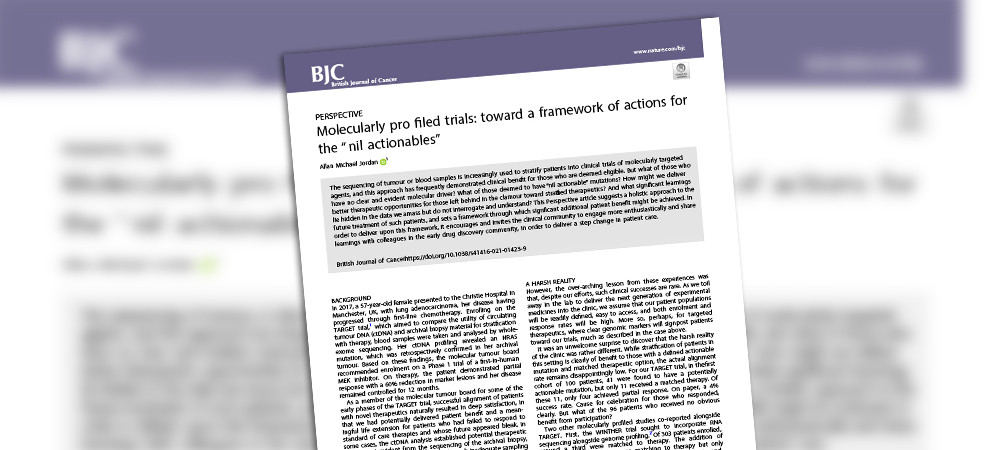
While there have been huge advances in cancer treatment in recent years, far too many solid tumours and blood cancers remain untreatable. Sygnature’s director of oncology drug discovery, Dr Allan Jordan, has published a ‘call to arms’ to the drug discovery and clinical communities in the British Journal of Cancer. He speculates that more, and better, cancer treatments might be found if discovery scientists and clinicians worked together more closely.
The approval of Novartis’s imatinib (Gleevec) back in 2001 ushered in a new era for cancer therapy. It was the first time that a specific genetic mutation within cancer cells had been targeted successfully, and provided the first effective treatment for chronic myelogenous leukaemia. This represented a huge advance on non-selective cytotoxic chemotherapy drugs, raising the prospect of being able to kill cancer cells without damaging healthy ones.
Since then, numerous other targeted cancer drugs have reached patients. Personalised medicine, where the drug is chosen based on disease genetics, is already proving a game-changer for some patients. It now costs less than $1000 to decipher the genetics of a tumour or blood cancer, and many key specific mutations can already be paired up with targeted drugs. Melanoma is just one example of a ‘difficult’ cancer that can now be treated – if the cells have the right mutation.
Yet, in practice, we remain a long way from being able to treat all – or even most – cancers in a genetically determined way. Today, only about 5% of patients benefit from the approach. For many others, their cancers simply don’t have a genetic profile that we understand. Even if they do, there is a good chance there is still no drug that specifically targets an identifiable mutation.
What should we be doing to find treatments for these patients? The answer may well lie in a closer collaboration between drug discovery scientists and their clinical colleagues, looking more deeply at those patients whose cancers are genetically unsuitable for either existing drugs or planned clinical trials. If we considered their genetics a little differently, we might be able to discover new cancer drug targets and medicines that would benefit more cancer types, and deliver another step-change in patient care.
Would you like to read on? We have made Allan’s BJC paper on the topic ‘open access’ so everyone can have a read, check it out:


Peak Proteins, NuChem Sciences, and SB Drug Discovery have now fully integrated with Sygnature Discovery.