

Ressources
-
STORM Therapeutics: From Lead to Pre-Candidate Nomination in 18 Months

STORM Therapeutics: From Lead to Pre-Candidate Nomination in 18 Months
Case study






Discover precise insights into brain neurochemistry with Sygnature Discovery's in vivo microdialysis and cOFM services. With over 20 years of expertise, we design bespoke studies that reveal how compounds modulate neurotransmitter systems in health and disease. Using UHPLC/HPLC with electrochemical detection or mass spectrometry, we deliver robust PK/PD data to support confident CNS decision making.




juillet 30, 2015

Inobrodib, an exciting, first-in-class oral anti-cancer drug in clinical development by CellCentric, was collaboratively designed, synthesised and supported on its pre-clinical journey by an integrated project team at Sygnature Discovery. Inobrodib is now showing promising results in Phase I and II trials for multiple myeloma and other cancer types.

Tenez‑vous au courant des dernières mises à jour de l’entreprise, des étapes clés et des annonces importantes.
Découvrez les conférences et rencontres scientifiques à venir, où vous pourrez échanger avec notre équipe.

Chez Sygnature Discovery, nous fournissons des solutions de découverte de médicaments de classe mondiale pour accélérer la progression de vos composés, de l’idée jusqu’à la clinique.

Notre équipe de direction rassemble une diversité d’expériences et de ressources, favorisant la collaboration et l’innovation dans l’ensemble du processus de découverte de médicaments.

Explorez les opportunités de carrière chez Sygnature Discovery. Rejoignez une équipe internationale qui obtient des résultats exceptionnels grâce à la collaboration, à l’innovation et à l’intégrité.
Inobrodib, an exciting, first-in-class oral anti-cancer drug in clinical development by CellCentric, was collaboratively designed, synthesised and supported on its pre-clinical journey by an integrated project team at Sygnature Discovery. Inobrodib is now showing promising results in Phase I and II trials for multiple myeloma and other cancer types.
Chez Sygnature Discovery, nous fournissons des solutions de découverte de médicaments de classe mondiale pour accélérer la progression de vos composés, de l’idée jusqu’à la clinique.
Notre équipe de direction rassemble une diversité d’expériences et de ressources, favorisant la collaboration et l’innovation dans l’ensemble du processus de découverte de médicaments.
Explorez les opportunités de carrière chez Sygnature Discovery. Rejoignez une équipe internationale qui obtient des résultats exceptionnels grâce à la collaboration, à l’innovation et à l’intégrité.
Focusing on the withdrawal phase of addiction, this article examines how behavioral pharmacology models assess drug dependence and therapeutic intervention in preclinical studies.
Prolonged exposure to a drug causes the body to adapt, resulting in drug users consuming higher quantities to experience the same effects, a process known as tolerance. When drug exposure is suddenly reduced or stopped, the physiological adaptations lead to withdrawal – a collection of unpleasant and sometimes dangerous symptoms.
A mild version of these symptoms can be observed in heavy caffeine (classified as mildly to moderate addictive) consumers who can be irritable in the morning until they’ve had a cup of coffee. This unpleasant experience can be alleviated by resuming drug use, reinforcing the addictive cycle. As a result, reducing withdrawal severity is a potential target for treating substance use disorders.
It is possible to model how the body adapts to prolonged drug exposure (dependence) and withdrawal in animal models. In contrast to intoxication models, withdrawal studies typically involve non-contingent drug administration, where a scientist administers the drug over an extended period.
When drug administration is abruptly stopped, a characteristic set of symptoms are induced which can be scored using manual observation or by video and behavioral analysis software.
Two critical factors must be carefully controlled when designing a preclinical withdrawal model:
Drug exposure during the dosing phase must remain high enough to induce physiological dependence. This can be achieved in several ways:
2. Ensuring drug exposure is stopped abruptly to trigger withdrawal
To induce this state, drug exposure must be stopped suddenly. This is straightforward for short half-like compounds, where cessation rapidly leads to declining drug levels.
However, challenges arise with long half-life drugs or osmotic pump delivery, where residual drug slowly tapers in the body, preventing overt withdrawal. In these cases, withdrawal can be pharmacologically precipitated by administering a drug that blocks the effect of the first drug. An example is using naloxone to block opioid receptors following morphine exposure.
While precipitated withdrawal can be effective, it introduced additional pharmacology that may not be ideal when assessing novel pharmaceutical treatments.
Preclinical models of dependence and withdrawal can be applied at two stages:
At Sygnature Discovery, we evaluated whether methadone would prevent rats from experiencing symptoms following prolonged morphine exposure. In the clinic, methadone is used as an opioid maintenance therapy, allowing people that have been using opioids, such as heroin and fentanyl, to transition to a safer opioid without experiencing severe withdrawal. We validated our model with a clinically relevant control so that it can be utilized in assessing efficacy of novel treatments.
To induce dependence, rats were administered with morphine (30 mg/kg) twice a day for 16 days. From day 17, rats were assigned to one of three treatment groups: continued morphine, saline, or methadone (20 mg/kg, twice daily). Throughout both the dosing and cessation phases, body weight, food and water intake were measured daily. In addition, a scientist observed each rat and scored a list of 45 behaviors daily.
Rats that were administered saline during the withdrawal phase consumed much more food (hyperphagia) and water (hyperdipsia) than rats not experiencing morphine dependence. They also showed behaviors that are linked to poor health and stress in rats.
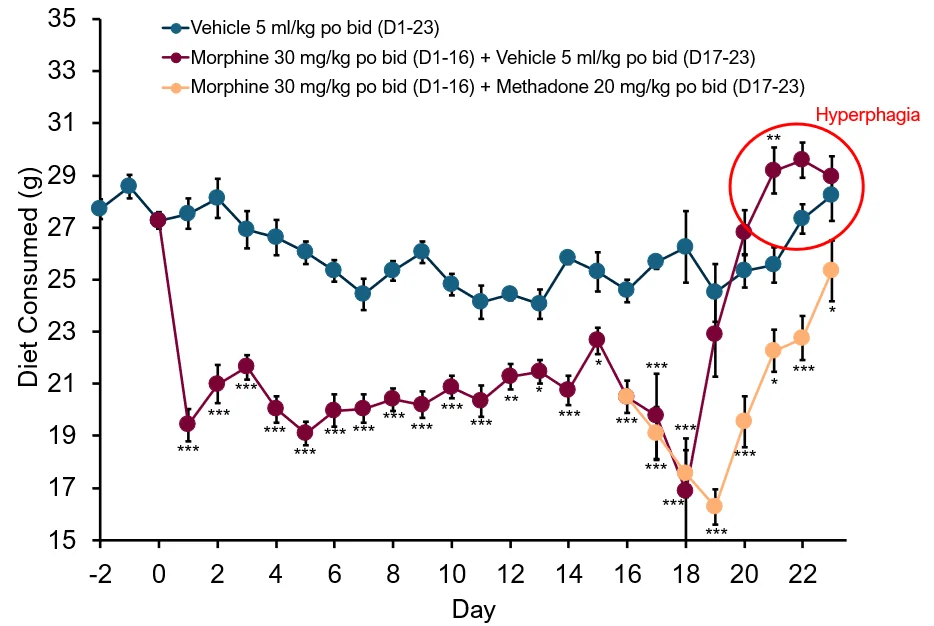
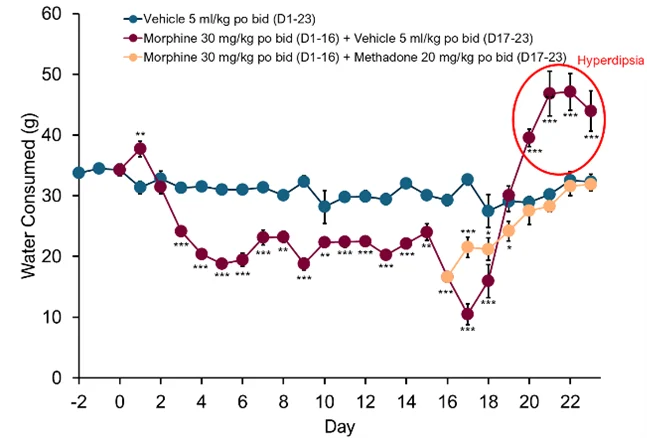
Daily diet and water consumption during baseline (vehicle treatment), induction of dependence (vehicle or morphine treatment) and withdrawal (vehicle or methadone treatment). Red circles highlight morphine withdrawal induced hyperphagia and hyperdipsia. *p<0.05, **p<0.01, ***p<0.001 versus vehicle.
In contrast, rats that were administered methadone during the withdrawal phase did not exhibit hyperphagia or hyperdipsia and behaviors linked to poor health and stress were reduced or absent. Similarly to methadone in the clinic, adverse effects such as decreased respiration were present. These effects are mediated in the clinic by starting treatment at a low dose and slowly increasing to a therapeutic dose.
Overall, these results confirm that methadone reduces opioid withdrawal symptoms in rats similar to the effect seen in humans.
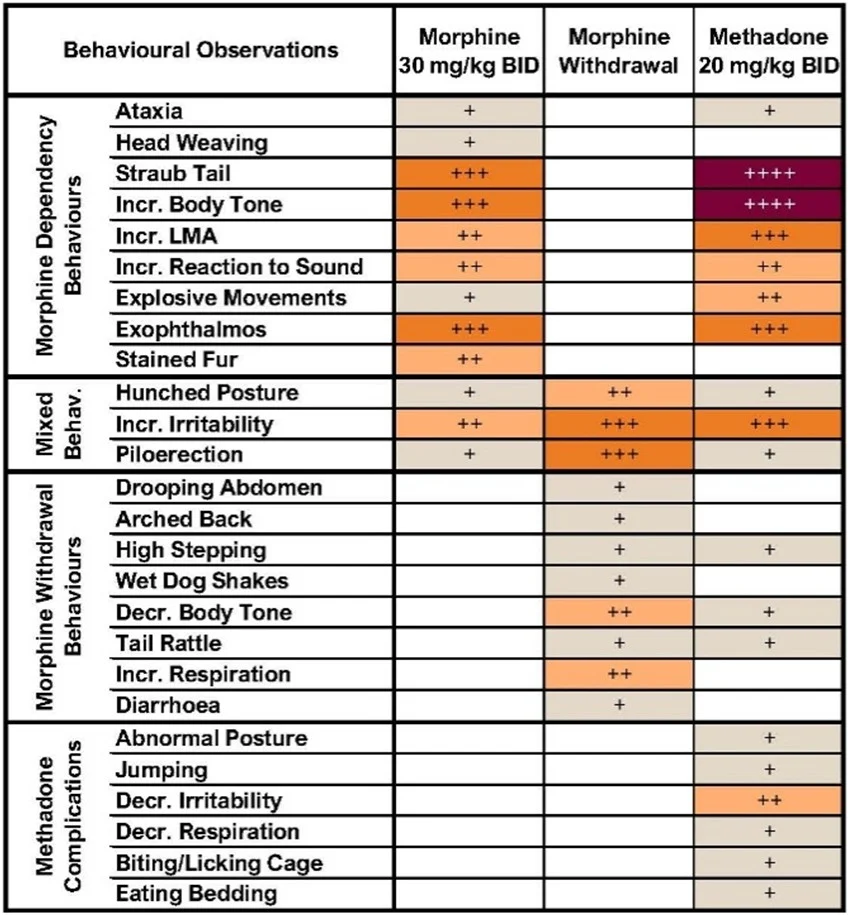
Behavioral observations during morphine dependence (morphine 30 mg/kg, twice daily) or morphine withdrawal, or morphine withdrawal with methadone treatment. Comparisons against vehicle by Wilcoxon Rank Sum test (all p<0.05-0.001). Mean score: +<0.025, ++0.25-0.49, +++0.5-0.74, ++++>0.75.
This article forms part of a four-part series exploring substance use disorders through the three-phase model of addiction and the preclinical behavioral pharmacology models used to support drug discovery.
Together, these articles examine how addiction develops, why it is so persistent, and how validated in vivo models are used to assess new therapeutic approaches.
An introduction to substance use disorders, the three-phase addiction model, and the role of behavioral pharmacology.
How reward-driven drug use and escalation are modelled in vivo.
Assessing dependence, withdrawal symptoms and maintenance therapies.
Understanding cue-induced relapse using reinstatement paradigms.

Focusing on the craving phase of addiction, this article examines how behavioral pharmacology models capture cue‑driven drug seeking and relapse vulnerability.
Addiction research depends on validated in vivo behavioral pharmacology models to assess reward, reinforcement, dependence and relapse-relevant behaviors.
These approaches form part of Sygnature Discovery’s CNS & pain in vivo pharmacology capabilities, supporting translational neuroscience and substance use disorder drug discovery from early research through to clinical decision-making.


Test