

Featured Resources
-
STORM Therapeutics: From Lead to Pre-Candidate Nomination in 18 Months

STORM Therapeutics: From Lead to Pre-Candidate Nomination in 18 Months
Case study
📣From lead to pre-candidate nomination in 18 months. Explore the STORM Therapeutics case study






Discover precise insights into brain neurochemistry with Sygnature Discovery's in vivo microdialysis and cOFM services. With over 20 years of expertise, we design bespoke studies that reveal how compounds modulate neurotransmitter systems in health and disease. Using UHPLC/HPLC with electrochemical detection or mass spectrometry, we deliver robust PK/PD data to support confident CNS decision making.




July 30, 2015

Inobrodib, an exciting, first-in-class oral anti-cancer drug in clinical development by CellCentric, was collaboratively designed, synthesised and supported on its pre-clinical journey by an integrated project team at Sygnature Discovery. Inobrodib is now showing promising results in Phase I and II trials for multiple myeloma and other cancer types.

At Sygnature Discovery, we deliver world-leading drug discovery solutions to accelerate your compound from idea to clinic.

Our leadership team brings diverse experience and insight, driving collaboration and innovation across drug discovery.

Explore careers at Sygnature Discovery and join a global team committed to science, collaboration, and integrity.
Inobrodib, an exciting, first-in-class oral anti-cancer drug in clinical development by CellCentric, was collaboratively designed, synthesised and supported on its pre-clinical journey by an integrated project team at Sygnature Discovery. Inobrodib is now showing promising results in Phase I and II trials for multiple myeloma and other cancer types.
At Sygnature Discovery, we deliver world-leading drug discovery solutions to accelerate your compound from idea to clinic.
Our leadership team brings diverse experience and insight, driving collaboration and innovation across drug discovery.
Explore careers at Sygnature Discovery and join a global team committed to science, collaboration, and integrity.
Focusing on the intoxication phase of addiction, this article examines how behavioral pharmacology models capture reward, reinforcement and binge‑like drug use in preclinical studies.
Substance use intoxication, often referred to as binge use, describes the phase in which a person consumes a drug for its rewarding and pleasurable effects often increasing the amount and frequency as time progresses. This is the phase that most people associate with addiction and the harm it can cause.
What begins as infrequent use can rapidly escalate as the body adapts to the drug’s effects. As tolerance develops, higher doses or more direct routes of administration (smoking and injection) are required to achieve the same reward. Preventing or reducing the rewarding effects of drugs, or making the experience unpleasant, is therefore a potential strategy for the treatment of drug addictions.
In animal models, intoxication can be modelled by making the drug freely available in drinking water or food or delivered only after a specific behavior has been performed. Due to the temporal nature of addition (rewards are most strongly recognized when they are instant), faster delivery of the drug to the brain produces a stronger association between the action and the reward. For this reason, models that deliver a drug intravenously are often more robust than models which deliver drugs orally.
Animals can be provided with continuous or limited access to a drug. Limited access models are frequently used to induce binge-like behavior, as unpredictable availability encourages animals to consume larger quantities over a short period of time. These models work particularly well for alcohol and palatable foods, such as chocolate in binge eating models.
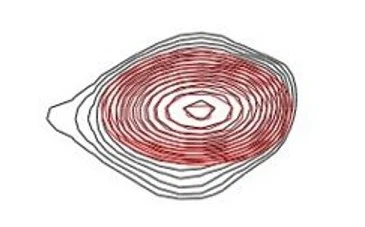
For example, when chocolate is made available to rats sporadically in 2-hour sessions, the amount of chocolate ingested in each session increases rapidly. The presence of the palatable reward also drives overeating of the standard chow drive that is always available.
Overeating is for pleasure rather than energy, and each session is followed by a period of consuming less standard diet. Such models allow researchers to assess whether novel pharmacotherapies reduce the amount of drug or palatable food consumed during each binge session.
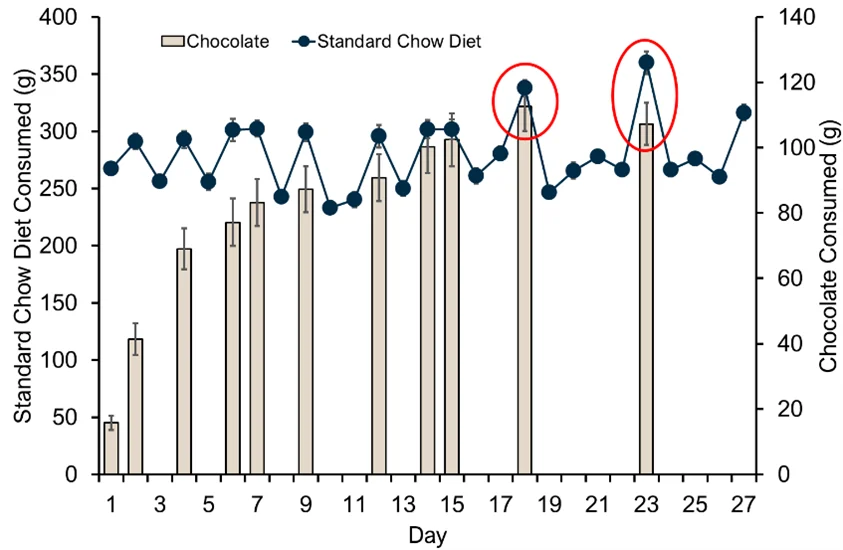
Consumption of standard chow diet (available ad libitum) and chocolate (available in 2-hour sessions) under a limited access binge model. Chocolate consumption becomes hedonic (not associated with metabolic need) and induces overeating of standard chow (red circles).
Another widely used approach involves requiring animals to perform a behavior to obtain the drug. Often the behavior required is pressing a lever or inserting their node into a hole. These operant self-administration models allow research to quantify the amount of work that an animal is willing to perform to obtain the drug.
The behavioral demand can easily be adjusted by increasing the number of responses required before drug delivery. This enables assessment of two critical questions:
Together, these measures provide insight into both reinforcement and motivation, key components of substance use disorders.
Self-administration, particularly intravenous self-administration, models have been used in preclinical safety testing since the 1960s to determine whether new drugs are likely to have abuse potential in humans. Therefore, there is a wealth of literature that demonstrates rodents and non-human primates will readily self-administer most drugs which humans find pleasurable, with the notable exception of psychedelics.
However, for these models to be useful in assessing novel pharmacotherapies for drug addictions, they must also demonstrate that current clinical interventions translate back into animals.
At Sygnature Discovery, we evaluated whether naltrexone, an FDA-approved treatment for opioid use disorder, would decrease heroin self-administration in rats. In the clinic, long-acting naltrexone implants reduce opioid use by blocking the rewarding and pleasurable effects. We validated our intravenous self-administration model with a clinically relevant control so that it can be utilized in assessing efficacy of novel treatments.
Rats were implanted with a jugular vein catheter for efficient drug delivery. Rats were then given daily access to a lever, which when pressed administers a small dose of heroin. Over several weeks, rats were self-administering approximately 17 doses of heroin within each 2-hour session.
To confirm that level pressing was drive by reward, heroin was replaced by saline. Within one week, the number of self-administered doses had reduced to less than 6 per session. When heroin was reintroduced, responding gradually returned to 17 self-administrations per session.
Finally, to assess pharmacological intervention, rats were administered with either vehicle or naltrexone (0.25, 1 or 2 mg/kg) 30 minutes before each session. Vehicle-treated rats continued to self-administer heroin as before. In contrast, rats treated with naltrexone showed a marked reduction in heroin intake. At 1 and 2 mg/kg, heroin self-administrations fell to 6 doses per session, similar to when they were receiving only saline.
These results demonstrate that naltrexone reduces heroin self-administration in rats, mirroring its clinical efficacy and validating this intravenous self-administration model for assessing novel treatments for opioid use disorder.
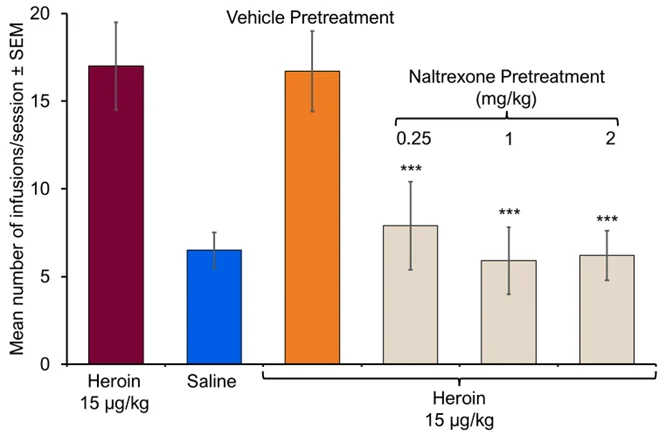
Mean number of infusions received per session when lever pressing provides; 1) heroin 2) saline 3) heroin following vehicle pre-treatment 4) heroin following naltrexone (0.25, 1 & 2 mg/kg) pre-treatment. ***p<0.001 versus vehicle pre-treatment.
This article forms part of a four-part series exploring substance use disorders through the three-phase model of addiction and the preclinical behavioral pharmacology models used to support drug discovery.
Together, these articles examine how addiction develops, why it is so persistent, and how validated in vivo models are used to assess new therapeutic approaches.
An introduction to substance use disorders, the three-phase addiction model, and the role of behavioral pharmacology.
How reward-driven drug use and escalation are modelled in vivo.
Assessing dependence, withdrawal symptoms and maintenance therapies.
Understanding cue-induced relapse using reinstatement paradigms.

Focusing on the withdrawal phase of addiction, this article examines how behavioral pharmacology models assess drug dependence and therapeutic intervention in preclinical studies.
Addiction research depends on validated in vivo behavioral pharmacology models to assess reward, reinforcement, dependence and relapse-relevant behaviors.
These approaches form part of Sygnature Discovery’s CNS & pain in vivo pharmacology capabilities, supporting translational neuroscience and substance use disorder drug discovery from early research through to clinical decision-making.




Peak Proteins, NuChem Sciences, and SB Drug Discovery have now fully integrated with Sygnature Discovery.
